Detect nr-axSpA and know that you can find this foe.
References: 1. Rudwaleit M, van der Heijde D, Landewé R, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis. 2009;68(6):777-783.
2. Protopopov M, Poddubnyy D. Radiographic progression in non-radiographic axial spondyloarthritis. Expert Rev Clin Immunol. 2018;14(6):525-533.
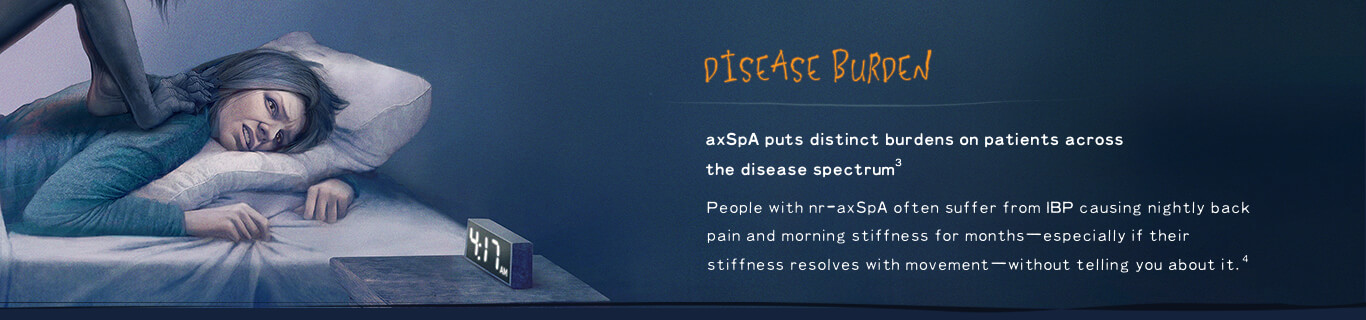
3. Mease PJ, van der Heijde D, Karki C, et al. Characterization of patients with ankylosing spondylitis and nonradiographic axial spondyloarthritis in the US-based Corrona Registry. Arthritis Care Res (Hoboken). 2018;70(11):1661-1670.
4. Strand V, Singh JA. Evaluation and management of the patient with suspected inflammatory spine disease. Mayo Clin Proc. 2017;92(4):555-564.
5. Kiltz U, Baraliakos X, Karakostas P, et al. Do patients with non-radiographic axial spondylarthritis differ from patients with ankylosing spondylitis? Arthritis Care Res (Hoboken). 2012;64(9):1415-1422.
6. Malaviya AN, Kalyani A, Rawat R, Gogia SB. Comparison of patients with ankylosing spondylitis (AS) and non-radiographic axial spondyloarthritis (nr-axSpA) from a single rheumatology clinic in New Delhi. Int J Rheum Dis. 2015;18(7):736-741.
7. Boonen A, Sieper J, van der Heijde D, et al. The burden of non-radiographic axial spondyloarthritis. Semin Arth Rheum. 2015;44(5):556-562.
8. Sepriano A, Landewé R, van der Heijde D, et al. Predictive validity of the ASAS classification criteria for axial and peripheral spondyloarthritis after follow-up in the ASAS cohort: a final analysis. Ann Rheum Dis. 2016;75(6):1034-1042.
9. van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis: a proposal for modification of the New York criteria. Arthritis Rheum. 1984;27(4):361-368.
10. Vidal C, Lukas C, Combe B, et al. Poor efficacy of TNF inhibitors in non-radiographic axial spondyloarthritis in the absence of objective signs: a bicentric retrospective study. Joint Bone Spine. 2018;85(4):461-468.
11. Chakrabarty S, Zoorob R. Fibromyalgia. Am Fam Physician. 2007;76(2):247-254.
12. Sieper J, Rudwaleit M. Early referral recommendations for ankylosing spondylitis (including pre-radiographic and radiographic forms) in primary care. Ann Rheum Dis. 2005;64(5):659-663.
13. Lee W, Reveille JD, Davis JC Jr, Learch TJ, Ward MM, Weisman MH. Are there gender differences in severity of ankylosing spondylitis? Results from the PSOAS cohort. Ann Rheum Dis. 2007;66(5):633-638.
14. Cross MJ, Smith EU, Zochling J, March LM. Differences and similarities between ankylosing spondylitis and rheumatoid arthritis: epidemiology. Clin Exp Rheumatol. 2009;27(4 suppl 55):S36-S42.
15. Chen HH, Chen TJ, Chen YM, Ying-Ming C, Chen DY. Gender differences in ankylosing spondylitis-associated cumulative healthcare utilization: a population-based cohort study. Clinics (Sao Paulo). 2011;66(2):251-254.
16. De Winter JJ, van Mens LJ, van der Heijde D, Landewé R, Baeten DL. Prevalence of peripheral and extra-articular disease in ankylosing spondylitis versus non-radiographic axial spondyloarthritis: a meta-analysis. Arthritis Res Ther. 2016;18:196.
17. Lories RJ, Baeten DL. Differences in pathophysiology between rheumatoid arthritis and ankylosing spondylitis. Clin Exp Rheumatol. 2009;27(4 suppl 55):S10-S14.
18. Ward MM, Deodhar A, Akl EA, et al. American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network 2015 recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Care Res. 2016;68(2):151-166.
19. Rudwaleit M, van der Heijde D, Khan MA, Braun J, Sieper J. How to diagnose axial spondyloarthritis early. Ann Rheum Dis. 2004;63(5):535-543.
20. Poddubnyy D, Rudwaleit M, Haibel H, et al. Rates and predictors of radiographic sacroiliitis progression over 2 years in patients with axial spondyloarthritis. Ann Rheum Dis. 2011;70(8):1369-1374.
21. Ablin JN, Eshed I, Berman M, et al. Prevalence of axial spondyloarthritis among patients with fibromyalgia: a magnetic resonance imaging study with application of the Assessment of SpondyloArthritis international Society classification criteria. Arthritis Care Res (Hoboken). 2017;69(5):724-729.
22. O'Dwyer T, McGowan E, O'Shea F, Wilson F. Physical activity and exercise: perspectives of adults with ankylosing spondylitis. J Phys Act Health. 2016;13(5):504-513.